"This clinical practice guideline synthesizes current best-evidence into four recommendations for [NHF] use..."
- Rochwerg et al. Intensive Care Med. 2020.1
Nasal High Flow (NHF) therapy is recommended for use in several applications by published guidelines. A clinical practice guideline for NHF use as a respiratory strategy in adult patients requiring respiratory support was recently published in Intensive Care Medicine,1 the official journal of The European Society of Intensive Care Medicine (ESICM).
Summary
A multinational panel of experts examined the body of NHF evidence and made these recommendations for its use compared to conventional oxygen therapy (COT)1:
Strong recommendation for primary respiratory support in acute hypoxemic respiratory failure.
Conditional recommendation for primary respiratory support in post-cardiothoracic surgery patients with obesity and/or high risk of postoperative respiratory complication.
No recommendation for pre-oxygenation of patients being intubated in the ICU (with a suggestion to continue NHF to pre-oxygenate those already receiving it).
Conditional recommendation for post-extubation respiratory support following extubation in those intubated for more than 24 hours and with any one or more feature of high risk of post-extubation failure.
Acute hypoxemic
respiratory failure
For primary respiratory support compared to COT.
Recommendation made with moderate certainty.
Strong
Recommendation
Recommendation made with moderate certainty.
Conditional Recommendation
NHF during intubation should be continued for patients who are already receiving NHF.*
Continue NHF*
respiratory failure
Recommendation made with moderate certainty.
Conditional Recommendation
Interpreting the strength of recommendations
Interpretation of the strength of the recommendations was provided for clinicians:
Strong recommendation
Most individuals should receive the recommended course of action. Adherence to this recommendation according to the guideline could be used as a quality criterion or performance indicator.
Formal decision aids are not likely to be needed to help individuals make decisions consistent with their values and preferences.
Conditional recommendation
Different choices are likely to be appropriate for different patients and therapy should be tailored to the individual patient’s circumstances. Those circumstances may include the patient or family’s values and preferences.
Implementation
“There is broad evidence that there is a substantial gap between the healthcare that patients receive and the practice that is recommended - also known as the research-practice gap, evidence-practice gap or knowing-doing gap. Evidence suggests that it sometimes takes more than a decade to implement research results in clinical practice...” Kristensen et al. BMC Health Services Research. 2016.2
It is important that awareness of the guidelines and adoption of the recommendations are advocated amongst the clinical community so that clinical practice continues improving and patients receive recommended care.
The clinical practice guideline highlights the cost effectiveness of NHF compared to COT for acute hypoxemic respiratory failure:
“Cost-effectiveness data suggests a net cost savings with [NHF] compared to COT in the range of 500–1000 British Pounds per patient (600–1200 US Dollars or Euros [equivalent currency]). This cost-effectiveness considers both the cost of the equipment but also the cost savings in intubations avoided. Consequently, [NHF] was judged by the panel to be associated with at least moderate cost savings.”
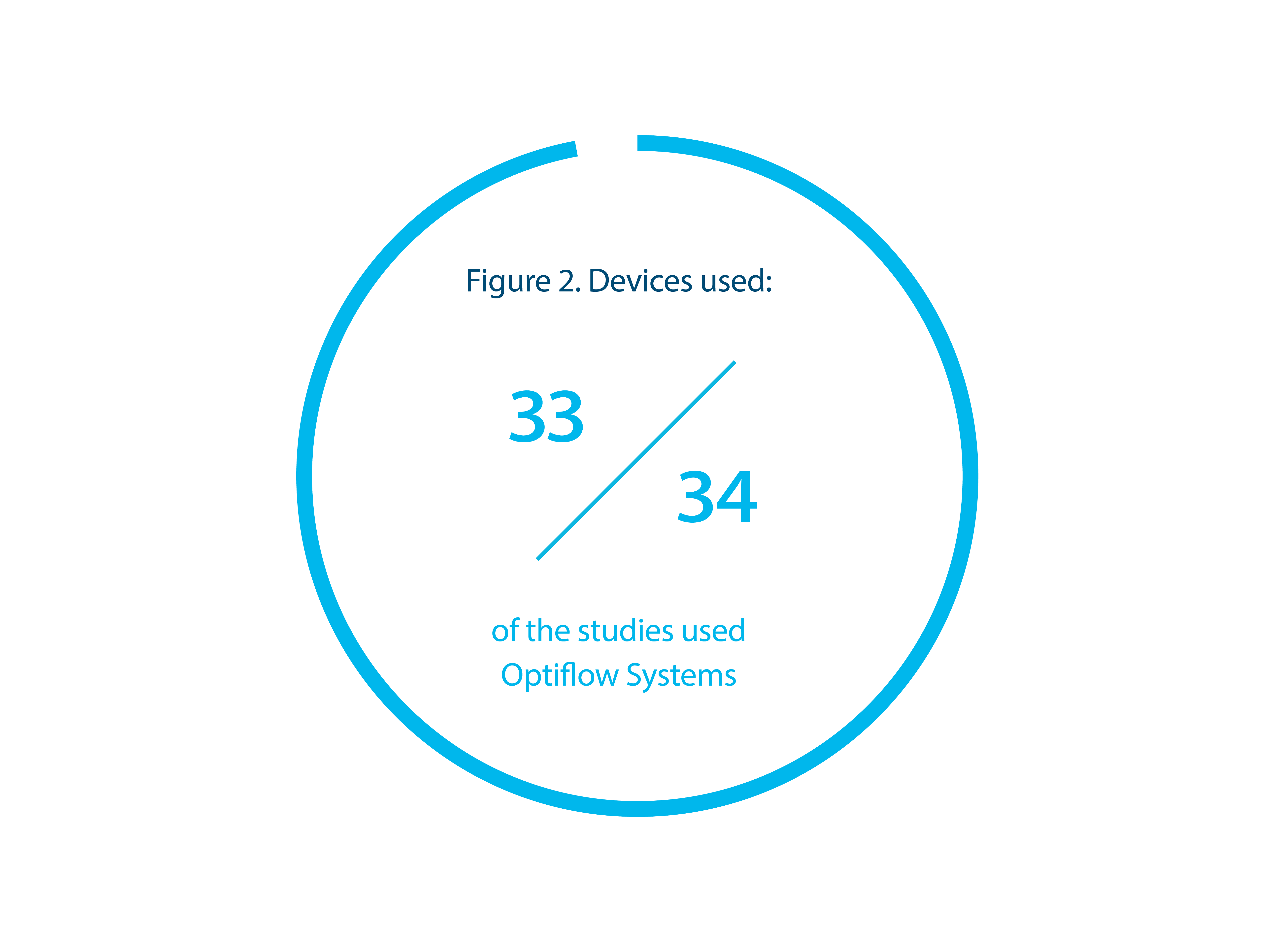
The systematic reviews with meta analyses supporting the clinical practice guidelines3-6 analyzed data from 34 published studies (mostly RCTs)7-40 and one study abstract.41 A review by Fisher & Paykel Healthcare showed that of the 34 published and analyzed studies, 33 used F&P Optiflow Systems, including a F&P Optiflow patient interface and a F&P humidity delivery system with humidity setting of 37 °C. See Figure 2. When selecting a NHF system, it is important to ensure the entire system, including device capabilities such as flow rate and humidity delivery, can provide the therapy to deliver the expected outcomes proven in the clinical body of evidence.
Definitions
F&P Optiflow System: A F&P purpose-built system for NHF – either an Airvo™ Optiflow System or a non-Airvo Optiflow System.
Airvo Optiflow System: A F&P Airvo with integrated flow source, humidifier and humidity delivery kit (F&P heated breathing tube and F&P auto-fill chamber). Used with a F&P Optiflow patient interface and able to accompany the patient throughout the hospital independent of medical air supply. Note that Airvo 2’s intended use is for spontaneously breathing patients only.
Non-Airvo Optiflow System: A F&P humidifier (e.g. MR850 system) and humidity delivery system (F&P heated breathing tube and F&P auto-fill chamber). Used with a F&P Optiflow patient interface and an independent flow generator such as a HFNC-capable ventilator.