Summary
- NHF therapy using weight-based protocols is well established in pediatric care areas across the hospital, including the PICU, ED and other general care areas.1-14
- In the ED and in general care, early use of NHF is effective in managing infants and children with bronchiolitis and other causes of AHRF, especially in hospitals without an on-site ICU.
- In the PICU, the use of NHF as primary treatment in acutely ill children has shown to lower sedation use, nasal trauma and shorten the duration of PICU and hospital stay compared with CPAP.14
Review of the literature
A systematic search of the available literature shows there are over 220 peer-reviewed papers investigating the use of nasal high flow (NHF) therapy in infants and children. These figures exclude papers investigating the use of NHF in the neonatal population. Of these, 31 are randomized controlled trials (RCTs) – they compared NHF with standard oxygen therapy, continuous positive airway pressure (CPAP) and alternative treatments.
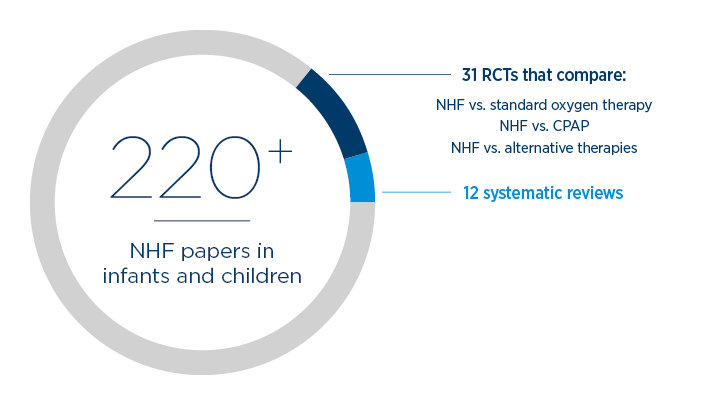
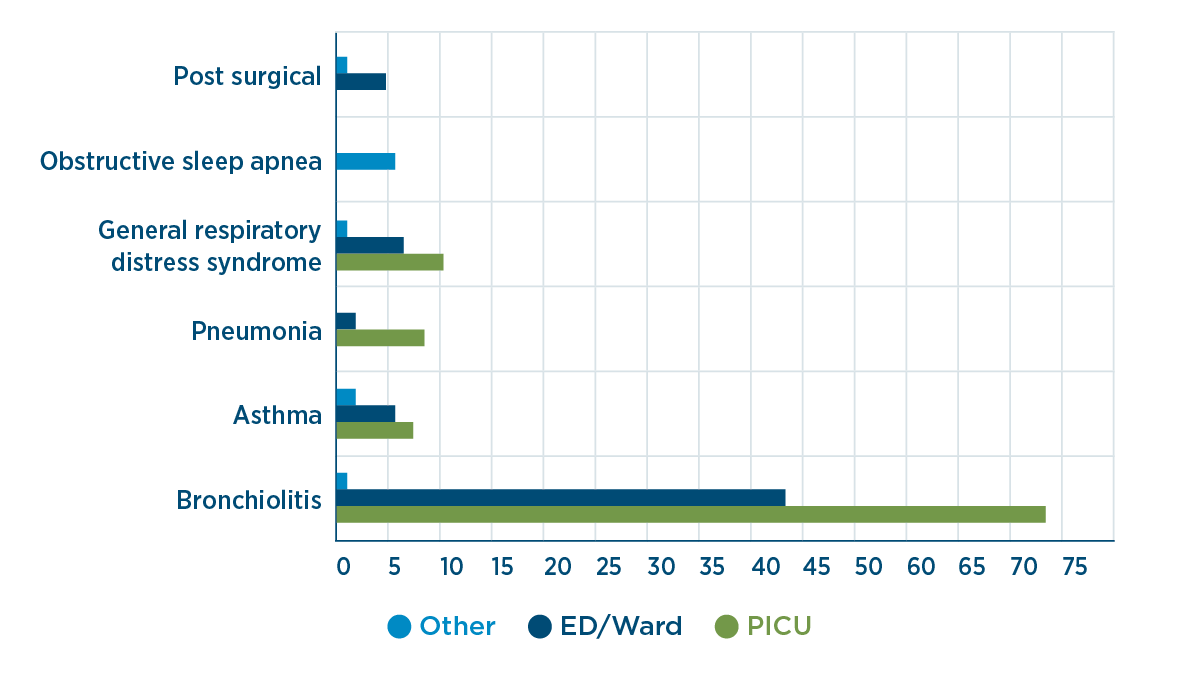
These studies represent application of NHF therapy in infants and children in a range of respiratory conditions in the pediatric intensive care unit (PICU), emergency department (ED) and other general care areas in the hospital.
The body of literature helps to define the role of NHF in pediatric respiratory care and supports:
- the use of NHF early in the course of respiratory distress, which is associated with improved physiological outcomes compared with standard oxygen therapy, including: 1-6
- improved breathing patterns and rapid unloading of the respiratory muscles
- significant reduction in the work of breathing
- rapid improvement to respiratory distress
- improved mucosal function and secretion clearance through the delivery of heated and humidified gas
- the early use of NHF outside of the PICU, either as primary support or early rescue therapy, can lead to reduced intubation rates and PICU admissions.7-11
Use of F&P Optiflow™ systems in RCTs
The weight of evidence is from studies which used an F&P Optiflow system, including an F&P Optiflow Junior interface and an F&P humidity delivery system.
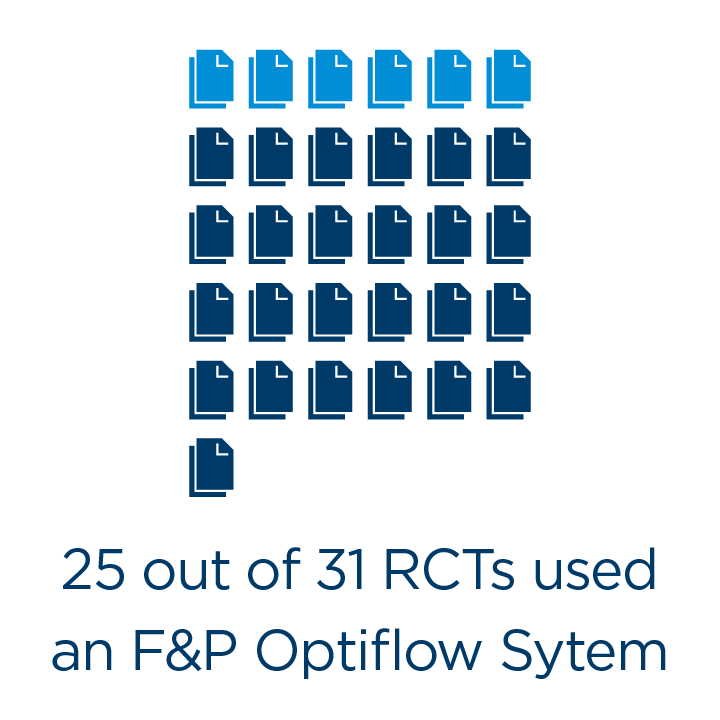
The systematic review conducted showed that 25 out of 31 RCTs (81%) used an F&P Optiflow system.
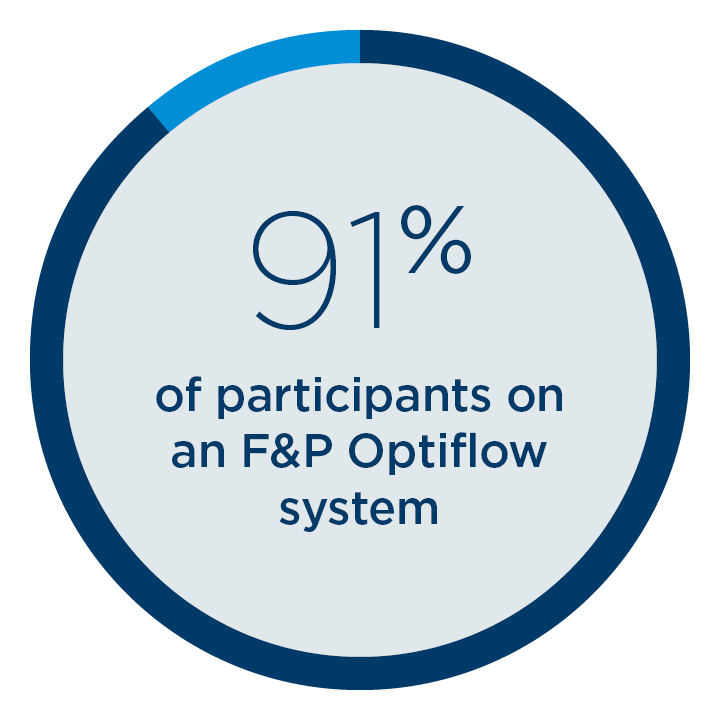
Of the 5,151 total participants on NHF in RCTs, 4,710
participants (91%) were treated using an F&P Optiflow system.
The PARIS trial
The largest NHF RCT was conducted by Franklin et al.1 This multi-center RCT supports the use of NHF in the ED and general care areas in young infants with bronchiolitis, and used the F&P Airvo™ with an Optiflow Junior interface.
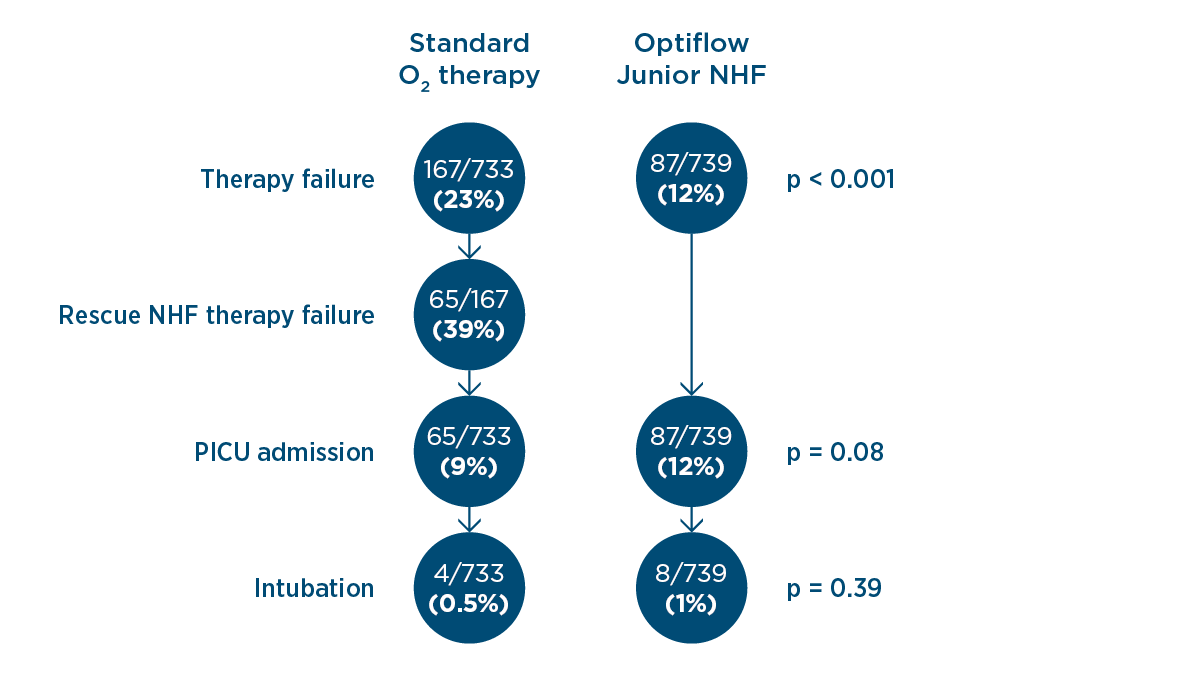
The primary outcome of the study was that the use of NHF at 2 L/kg/min as a primary treatment in the ED and general care areas resulted in a significantly lower rate of therapy failure compared with standard oxygen therapy (12 vs. 23%, p < 0.001). Therapy failure was defined as therapy escalation or PICU admission.

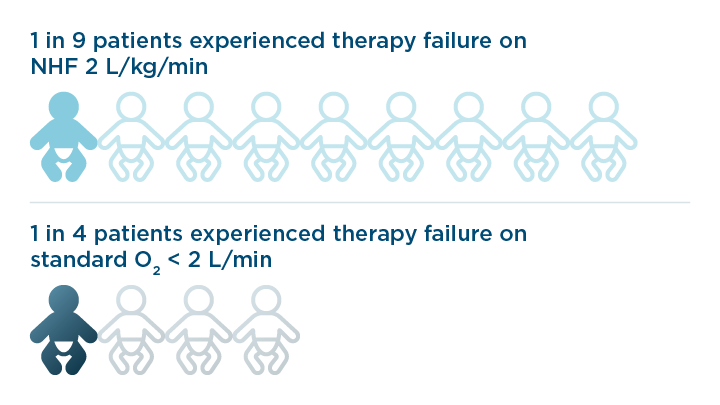
There were no significant differences between the secondary outcomes (PICU admissions, intubation rates and adverse events). It is important to note that the study design allowed patients on standard oxygen therapy who met the therapy failure criteria to escalate to NHF; 61% of the patients who failed on standard oxygen therapy were rescued by NHF and avoided PICU admission.
The PARIS 2 trial
This multi-center RCT, conducted by Franklin et al., addresses a current gap in the literature around the safety and efficacy of NHF in children with acute hypoxemic respiratory failure (AHRF) in the ED and general care areas.12
Primary outcome:
The hospital length of stay was longer in the NHF group compared with the standard oxygen therapy (SOT) group (NHF: 1.77 days vs. SOT: 1.50 days, p < 0.001).
Secondary outcomes:
ICU/HDU admissions were higher in the NHF group compared with the SOT group (NHF: 12.5% vs. SOT: 6.9%).
- Escalation of care in hospitals without on-site ICU/HDU was similar in both groups (NHF: 2.3% vs. SOT: 2.2%).
- The majority of the NHF patients admitted to the ICU remained on NHF and did not require therapy escalation (to noninvasive or invasive therapy).
NHF may have been perceived to be a higher level of respiratory support reserved for sicker children resulting in a lower threshold for escalation of care in hospitals with an on-site ICU.
Considerations for NHF practice and future research
PARIS 2 has provided insight into how infants and children with AHRF are managed and the many factors which influence care. These factors need to be considered when researching and protocolizing NHF in the pediatric population across the hospitals as ICU admissions, durations of oxygen support and hospital length of stay may be influenced.
NHF implementation
To reduce subjective clinical decision-making, there is a need for objective measures to determine therapy implementation and decision to escalate.
ICU admissions
ICU admissions can be driven by the availability of bed space and respiratory therapy prescribed rather than objective criteria.
Weaning
Lack of a consistent approach to weaning within hospitals and subjective decisions made by clinicians on patient therapy response may result in inconsistent weaning strategies.
What can we do to improve practice?
- Protocolize and standardize NHF using a multidisciplinary approach with intensivists, hospitalists and ED clinicians.
- Ensure there is a proactive initiation and weaning protocol in place using physiological parameters and therapy response through education or quality initiation projects.
- Education of clinicians and staff to ensure confidence and familiarity with NHF. This will allow effective management of children receiving NHF in the ED and general care areas, especially when ICU resources are scarce (pandemic, respiratory syncytial virus (RSV) surges etc).
The FIRST-ABC Trial
First-line Support for Assistance in Breathing in Children (FIRST-ABC) was designed as a master protocol of two pragmatic noninferiority RCTs by Ramnarayan et al.13
These RCTs investigated the safety and efficacy of NHF and CPAP when used as:
Post-extubation support in critically ill children (Step down)
First-line support in acutely ill children (Step up)
| Treatment Algorithm. A standardized treatment protocol was used to ensure the consistency of treatment across the multiple centers involved in the study. | ||||
| CPAP (7 – 8 cmH2O) or NHF starting at 2 L/kg/min → | Weaning therapy → | Stopping therapy → | Success: ≥ 48 hours free from respiratory support | Primary Outcome: Time to liberation from respiratory support |
Key findings
![]()
Step down
For post-extubation support in critically ill children
Patients in PICU transition to CPAP or NHF post-extubation. 553 participants (0 – 15 years, median age: 3 months). 22/28 PICUs in the UK.
When used for post-extubation, NHF did not meet noninferiority criteria compared with CPAP for time on respiratory support.
Patients on NHF required an average of 7.6 hours longer of respiratory support (NHF: 50.5 hours vs. CPAP: 42.9 hours; adjusted hazard ratio: 0.83 (95% CI: 0.70 – 0.99))
![]()
Step up
For first-line support in acutely ill children
Patients admitted to PICU receive CPAP or NHF as first-line therapy. 573 participants (0 – 15 years, median age: 9 months). 24/28 PICUs in the UK.
When used as first-line therapy, NHF met the noninferiority criteria when compared with CPAP for time on respiratory support.
Patients on NHF required an average of 5 hours longer of respiratory support (NHF: 52.5 hours vs. CPAP: 47.9 hours; adjusted hazard ratio: 1.03 (95% CI: 0.86 – 1.22))
Therapy failure occurred more frequently in the CPAP group compared with the NHF group.
Predominantly due to discomfort
Predominantly due to clinical deterioration
Of the secondary outcomes, the NHF group had significantly:
Lower use of sedation
NHF 27.7% vs. CPAP 37.0%
NHF 27.7% vs. CPAP 37.0%
Fewer occurrences of nasal trauma
NHF 2.0% vs. CPAP 6.5%
NHF 2.0% vs. CPAP 6.5%
Shorter mean duration of PICU stay
Mean difference -3.1 days
Mean difference -3.1 days
Shorter mean duration of acute hospital stay
Mean difference -7.6 days
Mean difference -7.6 days
![]()
Cochrane Review
Nasal high flow compared with standard oxygen therapy
The Cochrane Review on nasal high flow cannula therapy for infants with bronchiolitis, conducted by Armarego et al.16 in 2024, analyzed data from 16 trials. Of the 16 trials included, 11 assessed the effects of NHF therapy compared with SOT in treating infants with bronchiolitis. The PARIS trial was included in the analysis.
Primary outcomes:
The reduction in hospital length of stay with NHF was 15.6 hours.
Mean difference: 0.65 days lower (95% CI: 1.23 lower to 0.06 lower)
No differences in the incidence of adverse events.
Of the secondary outcomes, NHF compared with SOT had:
Improvement in respiratory rate
Mean difference: 6.34 bpm lower (95% CI: 11.39 lower to 1.29 lower)
Improvement in heart rate
Mean difference: 9.69 bpm lower (95% CI: 17.89 lower to 1.48 lower)
Reduction in instances to escalate
Risk ratio: 0.55 (95% CI: 0.39 to 0.79)
Reduction in duration of oxygen therapy
Mean difference: 0.59 days lower (95% CI: 1.00 lower to 0.18 lower)
Although the review also looked to compare NHF with CPAP, there were not enough studies to be able to demonstrate the efficacy of one therapy over the other. The evidence suggests that NHF is an effective treatment for infants with bronchiolitis.
Included studies were randomized controlled trials (RCTs) and quasi-RCTs using systematic methods of allocation, such as alternation, assignment based on date or birth, case record number and date of presentation. The research included papers up to December 2022.
An evidence-based approach to implementation of NHF in pediatric patients
This information collates data from published guidelines and the body of evidence. It does not overrule expert clinical judgment in individual patient management.
Flows
- 2 L/kg/min for patients up to 12 kg in weight has been shown to produce a rapid improvement in respiratory distress, and a reduced need for escalation of therapy.
- Flow rates for those over 12 kg have been protocolized by the PARIS12 and FIRST-ABC15 research groups.
| Weight (kg) | ≤12 | 13-15 | 16-30 | 31-50 | >50 |
| Starting flow rate | 2 L/min/kg | 25 – 30 L/min | 35 L/min | 40 L/min | 50 L/min |
Humidity
Heating and humidification of gases during respiratory support (including NHF and standard oxygen therapy):
- enables maintenance of airway defenses and mucociliary transport
- promotes efficient gas exchange
- reduces respiratory effort for the patient
- enables conservation of energy for growth and development.
O2
- PARIS 2 Protocol and FIRST-ABC group implemented the titration of FiO2 to achieve a target SpO2 of ≥ 92%.
Monitoring
- Non-responders can be identified within the first 60 minutes of NHF initiation, by the monitoring of physiological parameters such as heart rate, respiratory rate, and work of breathing.
Weaning off NHF therapy
ED (PARIS)
- Reduce the FiO2 to maintain SpO2 at target levels without reducing flow.
- Once the FiO2 has been reduced to 21% (room air) and the patient is stable at this concentration, NHF therapy can be stopped.
PICU (FIRST-ABC)
- When FIO2 < 40% and respiratory distress is not severe, use weaning flow rates
- When FIO2 < 30% and/or mild respiratory distress, stop NHF
| Weight (kg) | ≤12 | 13-15 | 16-30 | 31-50 | >50 |
| Weaning flow rate | 1 L/min/kg | 13 - 15 L/min | 18 L/min | 20 L/min | 25 L/min |
Definitions
F&P Optiflow system: An F&P system developed for the delivery of NHF. An F&P Optiflow interface (e.g., F&P Optiflow Junior 2) with either:
- an integrated flow source, humidifier and breathing set (e.g., F&P Airvo™ with AirSpiral™ tube and chamber kit)
- a separate flow source combined with an F&P humidifier and breathing set (e.g., MR850 and RT-series circuit kit).
Infants and children: This search included literature concerning the use of NHF in infants and children only, defined by the US Food and Drug Administration (FDA) as between 1 month to 2 years postnatal age and 2 to 12 years of age, respectively. Papers regarding the use of NHF in neonates (birth to 1-month postnatal) were not included, as indications for NHF are different in this population.
Nasal high flow (NHF): NHF is a mode of noninvasive respiratory support that delivers high flows of heated and humidified blended air and oxygen through an unsealed nasal interface.
Standard oxygen therapy: A form of oxygen therapy that is delivered through a nasal cannula at low flow rates (< 2 L/min) and is typically unheated and unhumidified. May also be referred to as conventional oxygen therapy.
Systematic search of the available literature: Conducted on July 21, 2022 using predefined search terms on PubMed, Embase & Cochrane Library, with data extraction and screening performed via DistillerSR (Evidence-Based Partners, Ottawa, Ontario) by internal F&P clinical researchers.
Cochrane Review:
A systematic review of clinical literature, meeting specified criteria to answer the question at hand. It is one of the best regarded forms of clinical evidence.
For further information, please view https://www.fphcare.com/hospital/infant-respiratory/nasal-high-flow/ or the hyperlinked references below.
If you have an enquiry about our products, please provide the following information so a Fisher & Paykel Healthcare representative can contact you. For further details on how this information will be used, see below or go to our privacy statement.